
 Prior studies suggest that Community Health Workers (CHWs) add significant value in healthcare settings. CHWs can improve physical health outcomes and lower health care costs for their patients, but there is limited research on the roles CHWs fill in behavioral health care.
Prior studies suggest that Community Health Workers (CHWs) add significant value in healthcare settings. CHWs can improve physical health outcomes and lower health care costs for their patients, but there is limited research on the roles CHWs fill in behavioral health care.
Trusted frontline health workers, CHWs often live in or come from the communities they serve. Importantly, they support hard-to-engage populations by liaising between patients and providers and by advocating for patient needs.
This qualitative study reviews the literature on CHWs in Certified Community Behavioral Health Clinics (CCBHCs). Additionally, the authors present findings from 12 interviews with staff at CCBHCs, CHW organizations, and state departments (including the Medicaid office), as well as one focus group with representatives from four CCBHCs.
Findings
- CCBHCs do not commonly employ CHWs. Some CCBHC staff were unfamiliar with the term CHW or were unclear about the roles and qualifications of the CHW workforce
- CHWs could likely help with many integrated care components. In particular, CHWs could help with warm handoffs to other care providers, following up with patients about their care plans, and connecting patients with complex care or social needs to relevant community-based services
- CCBHCs often experience staff shortages. Interviewees suggested that flexible, remote, and more appealing job opportunities outside of CCHBCs may be a reason for staff shortages
- CCBHCs have minimum education requirements for staffing. These requirements do not mention CHW certifications
- CCBHCs have complex administrative responsibilities as well as data and reporting requirements. So CHWs would need to fit into current workflows and job descriptions to fit the specific services that CCBHCs are required to provide
- Not all CCHBCs have systems to reimburse CHWs for the services they provide. Without the ability for CHWs to bill services to Medicaid, it is challenging for clinics to employ CHWs
Conclusions
Overall, CHWs could be a relatively low-cost and effective way to extend the behavioral health workforce, opening up a whole new pool of eligible candidates for employment in certain roles.
Expanding funding structures and assessing CCBHC staffing requirements could create a path toward including more CHWs in the workforce. Additionally, sharing information about the benefits of CHWs in CCBHCs may help to fill gaps in the behavioral health workforce.
Consideration of CHWs in CCBHCs is a timely issue with policy implications. In particular, many states are currently considering (or have recently passed) state-regulated CHW certifications or legislation to allow for the reimbursement of CHW services through Medicaid.

 In
In 
 Community Health Workers (CHWs) strive to bridge gaps between traditional healthcare providers and the communities they serve, but the community health worker profession faces several challenges to realizing its full potential. In the fall of 2017, the Center for Healthcare Research and Transformation (CHRT) published an
Community Health Workers (CHWs) strive to bridge gaps between traditional healthcare providers and the communities they serve, but the community health worker profession faces several challenges to realizing its full potential. In the fall of 2017, the Center for Healthcare Research and Transformation (CHRT) published an 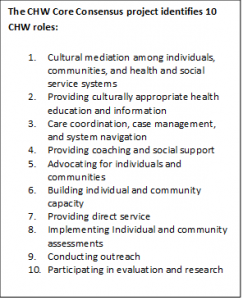 with patients, to improve healthcare and human service systems navigation, and to anticipate potential barriers to addressing health and social needs.
with patients, to improve healthcare and human service systems navigation, and to anticipate potential barriers to addressing health and social needs.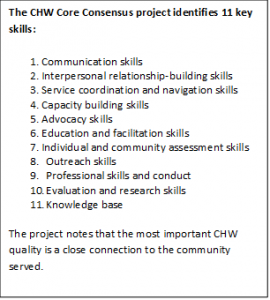 worker certification, 13 states have voluntary certification programs and 11 others are exploring the feasibility of statewide community health worker certification.
worker certification, 13 states have voluntary certification programs and 11 others are exploring the feasibility of statewide community health worker certification.